
Crowns vs. Inlays & Onlays: A Biomimetic Perspective
Biomimetic Dentistry
Dan Malloy DMD Restorative Dentist
Crowns vs. Inlays & Onlays:
Why Less Tooth Removal Is More
A biomimetic look at when a crown truly makes sense — and when a precision ceramic restoration can do the job better.
Patient Education Series· 8 min read· Restorative Dentistry
“You need a crown.” It’s one of the most common things dentists say — and one of the most misunderstood. But modern biomimetic dentistry asks a different question first: how much of your natural tooth can we save?
For decades, the full-coverage dental crown was the default answer to a weakened, cracked, or heavily decayed tooth. It’s reliable. It’s predictable. And it’s also one of the most aggressive procedures in dentistry — removing 60–75% of healthy tooth structure just to place a cap on top.
Biomimetic dentistry — a philosophy centered on mimicking the natural form and function of teeth — challenges this approach. Inlays and onlays, once seen as “half-measures,” are now understood to be biomechanically superior restorations in many situations.
Crown Prep

Onlay Prep
What Are Inlays and Onlays, Exactly?
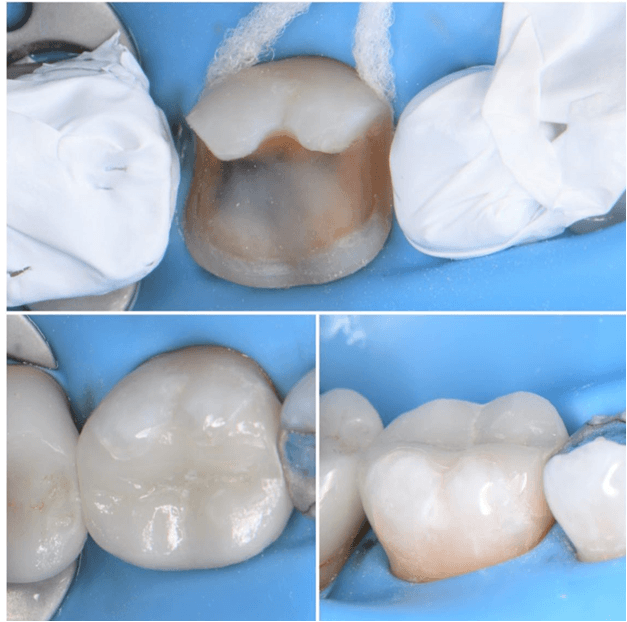
Think of an inlay as a precision-fitted puzzle piece. When a tooth has decay or damage confined to the area between its cusps (the pointed tips), a dentist removes only the compromised material and replaces it with a lab-crafted ceramic piece that fits perfectly into the cavity. It’s bonded in place and becomes structurally part of the tooth.
An onlay is essentially the same concept, but larger — it extends over one or more cusps when those areas are weakened or fractured. It’s sometimes called a “partial crown” because it covers more of the tooth surface, but unlike a crown, it only replaces what’s actually missing or damaged.
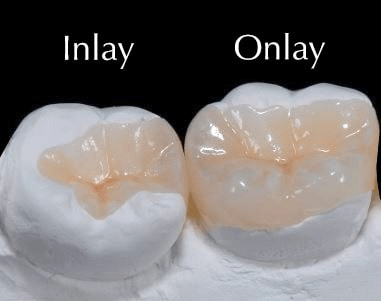
The inlay vs. onlay distinction
The line between them is purely anatomical. An inlay sits within the cusps — inside the chewing surface of the tooth. An onlay covers at least one cusp. Both are fabricated in a dental lab (or by CAD/CAM milling technology in-office) from ceramic, composite resin, or occasionally gold. Today, tooth-colored ceramics are overwhelmingly preferred for their esthetic integration and favorable bonding characteristics.
Biomimetic principle
Every millimeter of natural tooth structure you preserve is a millimeter that doesn’t need to be replaced artificially. Enamel — the outer layer of your tooth — is the hardest biological material in the human body. Once removed, it cannot regenerate. Protecting it is always the priority.
What’s Wrong with a Crown?
Nothing — when a crown is truly indicated. The problem is that crowns are often placed when a more conservative restoration would perform just as well, or better, and preserve far more healthy tooth.
Crown preparation requires aggressive reduction of all surfaces of the tooth — often healthy structure included.
Modern ceramic materials used in inlays and onlays are engineered to flex and compress much like natural enamel.
To place a crown, a dentist must shave down the entire tooth circumferentially — all sides, top, and slightly below the gumline — reducing it to a peg-like stub. Studies suggest this process removes an average of 63–72% of the original tooth structure. That’s not trimming the edges. That’s removing the majority of something that took years to grow and cannot be replaced.
Beyond the structural loss, there are functional consequences. A heavily prepared tooth is more vulnerable to thermal sensitivity. The reduced dentin layer provides less of a buffer to protect the pulp (the nerve). And research consistently shows that root canal treatment is more likely needed on crowned teeth than on teeth restored with bonded partial restorations.
63–72% Average tooth structure removed during crown preparation
3–5× Higher lifetime risk of root canal in crowned vs. inlay-restored teeth
90%+10-year survival rate for ceramic onlays in clinical studies
The Biomimetic Case for Inlays and Onlays
Biomimetic dentistry draws its principles from engineering and biology: materials and designs should mimic the natural behavior of what they replace. A healthy tooth is not rigid — it flexes microscopically under biting forces, with enamel and dentin acting as complementary layers that absorb and distribute stress.
When a full crown is placed, this natural stress-distribution system is disrupted. The crown material — whether zirconia, PFM, or even all-ceramic — behaves differently than enamel. This mismatch can transmit stress into the root and bone in ways the natural tooth was never designed to handle.
“The goal of biomimetic dentistry is not to replace the tooth — it is to restore it. Every restoration we place should work with the tooth’s biology, not against it.”— Academy of Biomimetic Dentistry
Biomimetic restorations are often placed under microscope magnification, allowing precise removal of only damaged tissue and perfect adaptation of the restoration.
Bonding changes everything
One of the most important advances enabling inlays and onlays to outperform crowns in many cases is adhesive bonding technology. Modern ceramic restorations are chemically bonded to tooth structure with resin cements that create a genuinely integrated interface. The restoration and the tooth move together, flex together, and share the stress of chewing.
Crowns, by contrast, historically relied on mechanical retention — the physical “grip” of cement holding a cap onto a prepped tooth. While modern cementation has improved, the fundamental relationship between crown and tooth is different: they are layered, not fused.
Why ceramic inlays & onlays feel natural
High-quality ceramic has a modulus of elasticity (stiffness) very close to natural enamel. When bonded properly, the restoration distributes biting force in a pattern nearly identical to an intact natural tooth — protecting the root, the bone, and the opposing teeth.
When a Crown Is Still the Right Answer
Biomimetic dentistry is not anti-crown. There are absolutely situations where a full-coverage crown is the correct, evidence-based choice. Honesty about those situations is part of what defines an ethical biomimetic approach. Some teeth have more extensive damage that require full coverage crowns.
If your dentist recommends a crown for a tooth with limited damage — particularly if you haven’t experienced pain and the tooth has never had significant work — it’s always reasonable to seek a second opinion from a dentist trained in biomimetic or adhesive dentistry. Not to delay necessary care, but to ensure you’ve explored every conservative option first.
What the Procedure Looks Like
For an inlay or onlay
- ✓ Local anesthetic is applied; only the decayed or damaged tissue is removed — healthy structure is untouched
- ✓ A digital scan captures the exact shape of the prepared cavity
- ✓ The ceramic restoration is milled or lab-fabricated to micron precision
- ✓ The piece is bonded in place with a resin cement that chemically integrates with the remaining enamel and dentin
- ✓ Bite is checked and refined; the finished restoration is virtually indistinguishable from natural tooth
For a crown (for comparison)
- ✗ All surfaces of the tooth are ground down, including healthy enamel — typically 1.5–2mm circumferentially
- ✗ A temporary crown is placed while the permanent one is fabricated — often two visits
- ✗ The permanent crown is cemented over the prepared stub; natural tooth sensation is altered
- ✗ Once the process is started, it is essentially irreversible — the tooth can never be un-prepped
Digital scanning technology allows precise fabrication of inlays and onlays with a fit that was impossible to achieve a generation ago
Questions to Ask Your Dentist
If a crown has been recommended for you, these questions will help you have a more informed conversation about your options:
- ? Is there enough healthy tooth structure remaining for an inlay or onlay? If so, why is a crown preferred?
- ? Is this tooth vital (does the nerve still have blood supply)? Vital teeth are far better candidates for conservative restorations.
- ? Where exactly is the fracture or decay? Ask to see the X-ray or photo, and ask what would be removed by each option.
- ? If we start with an onlay and it doesn’t work, can we still do a crown later? The answer is almost always yes — but the reverse is never true.
- ? Are you trained in adhesive/biomimetic dentistry? Bonded ceramic restorations require specific materials knowledge and technique that not all dentists have.
Our Philosophy: Treat the Tooth You Have
At our practice, we approach every damaged tooth with a single guiding question: what is the least invasive restoration that will give this patient the best long-term outcome? For the majority of teeth with moderate damage — even significant cusp loss — that answer is an onlay or inlay, not a crown.
We use high-magnification loupes to ensure that only damaged tissue is removed. We select ceramic materials matched to the optical and mechanical properties of natural enamel. And we take the time to explain every option, including the option to monitor rather than treat, when appropriate.
Your teeth are not expendable. Every millimeter we preserve is a millimeter that will still be there in 20 years — protecting the nerve, anchoring the root, and keeping your tooth feeling like your own.
Ready for a Second Opinion?
If you’ve been told you need a crown, we’ll review your records, X-rays, and exam findings and tell you honestly whether a more conservative option is appropriate. Schedule a Biomimetic Consultation
Or call us directly at 610-320-9993— we’re happy to answer questions before you book.
